

Are you prepared for Medicare's latest updates? Watch our on-demand webinar "Understanding Medicare's 2026 Changes to Remote Care Management."
***
Remote patient monitoring (RPM) has come a long way since it was formally introduced by the Centers for Medicare & Medicaid Services (CMS) in 2019. For practices, hospitals, health systems, federally qualified health centers (FQHCs) and rural health clinics (RHCs), RPM has become an essential tool for keeping patients connected between in-person visits and exams.
Yet the financial side of remote patient monitoring has not always matched clinical success, as many organizations have struggled to make the economics of RPM work. Vendors often promised rapid or guaranteed returns, but the ROI reality was more complicated. CMS’s reimbursement rules were rigid, patient adherence — and thus billable services — varied, and the administrative effort to stay compliant and get paid was significant.
At Prevounce Health, we encourage organizations to approach RPM ROI projections carefully. Real results depend on factors like strong workflows, accurate documentation, and educated and engaged patients.
The 2026 CMS Physician Fee Schedule (PFS) final rule has not diminished the importance of these elements, but it has changed the RPM equation in a few very positive ways. A higher conversion factor and new code flexibility make it easier than ever for compliant RPM programs to deliver measurable financial returns and expand the clinical value of the service to more patients.
History of RPM Reimbursement
When Medicare first began reimbursing for RPM, the intent was clear: reward providers for managing patients proactively between visits. The structure, however, was narrow. To bill for the device-supply code, CPT 99454, a patient had to generate at least 16 days of physiological data within a 30-day period. To bill for the management code, CPT 99457, care teams had to document at least 20 minutes of clinical staff time.
In practice, those thresholds excluded a wide range of real-world scenarios. Consider a Medicare patient enrolled in a GLP-1 weight-loss program who might only need to record a few weight readings each month. This data is valuable to the patient’s care team, yet enrolling them in RPM would not be financially sound given that they would not likely reach the 16-day data threshold required for reimbursement. Even a hypertension patient whose blood pressure had stabilized could benefit from limited (less than 16 days) monitoring, but their case would fall outside the strict billing rules. In addition, rural patients with inconsistent internet access may miss enough transmissions to lose RPM eligibility even if their health conditions would benefit from the ongoing monitoring service.
2026: Year of Increased Reimbursement
While these clinical limitations frustrated providers, and those patients who dropped out of programs due to non-compliance, so has changes to RPM payments. The Medicare conversion factor (CF), the multiplier CMS uses to translate relative value units (RVUs) into dollar amounts, has trended downward for several years. By 2025, it had reached $32.35, down close to $4 from 2020. Even well-run RPM programs found themselves squeezed between growing clinical need and shrinking reimbursement
Here is the historical trend in conversion factors since RPM was introduced:
|
Year |
Conversion Factor |
Notes |
|
2019 |
$36.04 |
Baseline year for comparison. |
|
2020 |
$36.09 |
A slight increase from 2019. |
|
2021 |
$34.89 |
A 3.3 % reduction due to budget-neutrality adjustments and expiration of a temporary fix. |
|
2022 |
$34.61 |
A slight decrease from 2021 |
|
2023 |
$33.89 |
About a 2% reduction from 2022. |
|
2024 |
$33.29 |
Reduced by 3.37 % from Jan-March, then partially offset by a 1.66% legislative update. |
|
2025 |
$32.35 |
Another 2.83% reduction. |
|
2026 |
$33.40 (non-APM) / $33.57 (APM) |
3.25% increase (non-APM) / 3.77% increase (APM). |
(Source: CMS Physician Fee Schedule and associated federal rulemaking summaries, 2019–2026.)
This largely consistent downward movement has placed pressure on providers who rely on time-based reimbursement. A lower CF means the same clinical effort is reimbursed at a lower rate, reducing the resources available to staff, monitor, and engage patients. This negative trend has also served to dissuade some providers from considering launching an RPM program. The 2026 PFS final rule reverses that trend. For the first time in several years, CMS actually raised the CF, marking a modest but meaningful step toward restoring economic balance to remote monitoring.
What Changed in the 2026 Physician Fee Schedule?
On Oct. 31, 2025, CMS released the 2026 PFS final rule, and the changes it solidifies are anything but routine. This rule introduces several policy revisions that directly affect remote patient monitoring and other remote-care services.
New RPM CPT Codes 99445 and 99470
First, CMS finalized two new codes — CPT 99445 and CPT 99470 — that expand RPM flexibility for providers and help strengthen ROI in the process.
RPM code 99445 covers 2 to 15 days of physiological data within a 30-day cycle. It will be reimbursed at the same rate in 2026 as 99454, which applies to 16 to 30 days. This single decision removes one of the most frustrating barriers in RPM billing. Providers can now support patients who only need short-term monitoring, such as those adjusting medication, recovering from surgery, or managing mild exacerbations, without forfeiting reimbursement.
RPM code 99470 covers 10 to 20 minutes of clinical staff time for RPM treatment management. It carries roughly half the 2026 reimbursement value of 99457, which continues to apply to 20 or more minutes of service. Just as significant, CMS chose not to reduce the reimbursement for existing 20-minute codes (99457 and 99458), preserving their full value for practices already delivering longer encounters.
These CPT code additions mark an important recognition that RPM encounters do not always fit neatly into the rigid 16-day and 20-minute thresholds that have governed billing until now. The new codes create space for shorter monitoring periods and partial-month management while maintaining financial parity with longer-duration services.
In addition, these updates close long-standing gaps between clinical effort and financial recognition. Shorter but meaningful patient interactions that once went uncompensated can now be documented and reimbursed appropriately. The result is a structure that rewards proactive engagement and aligns reimbursement with patient needs rather than arbitrary time or data thresholds.
Below is a graphic illustrating this updated RPM billing structure for 2026, reflecting the addition of two new CPT codes:
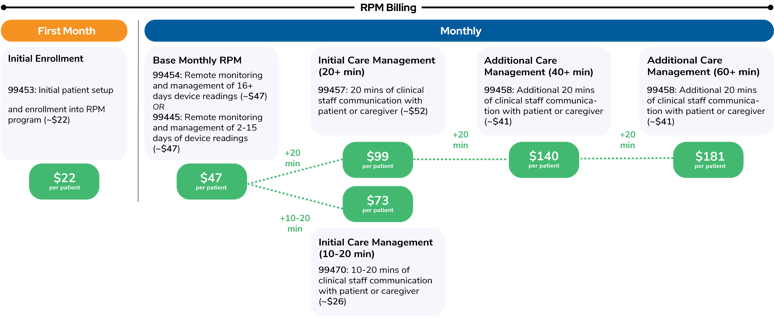
*Rates shown represent the estimated non-facility national averages for non-AMP .
For a deeper look at how to bill for RPM services, download our 2026 RPM Billing guide.
For years, professional organizations such as the American Medical Association have urged CMS to make these very changes. They argued that RPM deserves the same flexibility as traditional evaluation and management (E&M) services, since the clinical work is comparable and the outcomes are often superior. The 2026 final rule represents a tangible shift toward that goal, pairing clinical flexibility with improved financial stability.
Increased Conversion Factor
Second, as discussed earlier, CMS raised the conversion factor for the first time in years. The 2026 CF is $33.57 for qualifying alternative payment model (APM) participants (QPs) and $33.40 for non-QPs, both increases of more than 3% over 2025. This is also the first year CMS has established two separate conversion factors, signaling a shift toward differentiated reimbursement for value-based participants versus fee-for-service providers. The increase reverses a five-year pattern of reductions and provides meaningful relief across time-based codes such as RPM and chronic care management (CCM).
RVU Efficiency Adjustment
Third, the 2026 final rule finalizes a 2.5% “efficiency adjustment” to work RVUs for non–time-based services. While this adjustment does not affect RPM codes, it reinforces CMS’s broader emphasis on paying for clinician time, care coordination, and longitudinal outcomes rather than procedural volume.
Incorporation of Hospital Cost Structures
Finally, CMS made an unexpected decision concerning how it sets relative values. The agency announced that hospital outpatient department (HOPD) data will now help determine rate-setting for certain technical services, including some remote monitoring activities. This is a departure from both historical CMS methodology and the AMA’s recommendations, which have long relied on physician practice expense data as the standard. By incorporating hospital cost structures, CMS is signaling a new approach — one that ties reimbursement more closely to real-world resource use rather than the AMA’s traditional modeling assumptions.
What This Means for RPM ROI in Practice
To see what these changes could mean for ROI on a remote patient monitoring program in 2026, consider a clinic in Upstate New York running an RPM program for 522 patients with hypertension and diabetes.
In June 2025, most patients met the 16-day and 20-minute thresholds, but not all. Sixteen percent of participants (83 patients) recorded between 2 and 15 readings in the month. Another 6% (31 patients) received between 10 and 20 minutes of staff time. Those encounters represented real clinical work, but under 2025 rules they generated no reimbursement. Here’s a side by side comparison of 2025 revenue compared to 2026 forecasted revenue (assuming no new patients are added and all other variables remain the same):
.png?width=384&height=727&name=2026%20reimbursement%20increase%20example%20-%20vertical%20(1).png)
Consider the same patients and same clinical services rendered in 2026, with the only change being the new billing structure. The program’s annual revenue would rise by roughly $101,124. In addition, expanded coverage would likely encourage the clinic to assess its patients and enroll more of them into the RPM program because of the valuable services now covered under the new CPT codes. This is the kind of clinical and financial policy alignment providers have long been waiting and pushing for.
Capitalizing on the New RPM Opportunities
Healthcare leaders with remote patient monitoring programs should not wait until January to act on these significant changes. Identify patients who aren’t enrolled in remote care but could benefit from shorter interactions and 2-15 days of data transmission. This is a good time to begin educating these patients on RPM and preparing to enroll them in the new year. Next, review your billing systems so the new codes can be activated quickly once finalized. Train your teams to document short interactions accurately, and make sure virtual supervision is reflected in your compliance protocols. Assure that your vendor is prepared to meet your needs.
The Bottom Line on RPM ROI in 2026
The latest CMS PFS final rule is a clear step forward for remote patient monitoring. It rewards the time, technology, and attention that go into modern remote care. By raising the conversion factor and introducing RPM CPT codes that better reflect real patient engagement, CMS has brought the reimbursement structure closer to clinical reality.
For providers that already run effective RPM programs, these updates could transform financial sustainability. For those still on the sidelines, 2026 is the year when the ROI makes even more sense. Book a consultation with one of our remote care management experts to learn how RPM can improve your bottom line in 2026.
CPT Copyright 2025 American Medical Association. All rights reserved.
CPT® is a registered trademark of the American Medical Association.
Disclaimer:
Health economic and reimbursement information provided by Prevounce is gathered from third-party sources and is subject to change without notice as a result of complex and frequently changing laws, regulations, rules, and policies. This information is presented for illustrative purposes only and does not constitute reimbursement or legal advice.
Prevounce encourages providers to submit accurate and appropriate claims for services. It is always the provider’s responsibility to determine medical necessity, the proper site for delivery of any services, and to submit appropriate codes, charges, and modifiers for services rendered. It is also always the provider’s responsibility to understand and comply with Medicare national coverage determinations (NCD), Medicare local coverage determinations (LCD), and any other coverage requirements established by relevant payers which can be updated frequently.
Prevounce recommends that you consult with your payers, reimbursement specialists, and/or legal counsel regarding coding, coverage, and reimbursement matters.
Payer policies will vary and should be verified prior to treatment for limitations on diagnosis, coding, or site of service requirements.
The coding options listed here are commonly used codes and are not intended to be an all- inclusive list. We recommend consulting your relevant manuals for appropriate coding options.
The Health Care Provider (HCP) is solely responsible for selecting the site of service and treatment modalities appropriate for the patient based on medically appropriate needs of that patient and the independent medical judgment of the HCP.