Updated November 4, 2025
Chronic care management (CCM) is a Centers for Medicare & Medicaid Services’ (CMS) program designed to help healthcare providers deliver proactive, coordinated care to patients with two or more chronic conditions. This program entails structured care plans, regular check-ins, and better care coordination between providers — helping ensure patients receive the ongoing support they need to effectively manage their conditions. CCM also creates reimbursement incentives to support practices in their efforts to deliver more engaging, proactive care that can help reduce hospitalizations and other potentially avoidable and expensive medical services.
Providers must understand and and correctly use the proper CCM CPT codes to ensure CMS compliance and receive appropriate reimbursement for the services. In this guide, we’ll focus on one of the CCM CPT codes: 99439. We’ll examine what CPT code 99439 entails, who can bill for it, patient eligibility criteria, billing requirements, and best practices for achieving seamless integration of the services covered under 99439 into your CCM program.
What Is CPT Code 99439?
CPT 99439 is an add-on non-complex chronic care management code that reimburses providers for additional clinical staff time beyond the initial 20 minutes already covered under CPT 99490. Specifically, 99439 covers each additional 20 minutes of non-face-to-face CCM services provided monthly, directed by a physician or other qualified healthcare professional (QHP). CPT 99439 helps providers deliver comprehensive care coordination, ongoing patient monitoring, and proactive chronic condition management.
In 2026, CPT code 99439’s national average non-facility reimbursement rate is about $50.
Who Can Bill for CPT 99439?
CMS authorizes billing of CPT 99439 by the same healthcare providers eligible to bill CPT 99490, including:
- Physicians (MDs)
- Certified nurse midwives (CNMs)
- Clinical nurse specialists (CNSs)
- Nurse practitioners (NPs)
- Physician assistants (PAs)
General Supervision
Like CPT 99490, CPT 99439 services provided by clinical staff fall under the category of “general supervision” by the billing practitioner. Under general supervision, the billing practitioner oversees and directs chronic care management services but does not need to be physically present during service delivery. Clinical staff may be employees or contracted professionals performing tasks as extensions of the billing provider.
CMS classifies CCM codes like CPT 99439 under general supervision within the Medicare Physician Fee Schedule (PFS), ensuring flexibility in service delivery and compliance with Medicare guidelines. Clinical staff can manage CCM services effectively as long as state laws, licensure, and scope of practice requirements are met, thereby extending providers' care management and billing capabilities.
How Often Can 99439 Be Billed?
CPT 99439 can be billed monthly as an add-on to CPT 99490. Providers may bill up to two units of 99439 per calendar month, with each unit representing an additional 20-minute increment of clinical staff time.
Patient Eligibility for CPT 99439
Patients must meet standard CCM eligibility requirements to qualify for CPT 99439 billing, including:
- Having two or more chronic conditions expected to persist at least 12 months or until death.
- Conditions posing significant risk for death, acute exacerbation, or functional decline.
Common conditions eligible for CPT 99439 services include the following:
- Hypertension
- Diabetes
- Chronic heart failure (CHF)
- Chronic obstructive pulmonary disease (COPD)
- Asthma
- Cardiovascular disease
- Depression
Note: To learn more about CCM patient eligibility, download this guide.
Billing Requirements for CPT 99439
To receive reimbursement and ensure compliance with CMS regulations, providers and billers must understand the billing requirements for CPT 99439. Adhere to the following requirements when billing CPT 99439:
- Initial visit: New CCM patients or those not seen within the past year must have a face-to-face initiating visit during an E/M visit, annual wellness visit (AWV), or initial preventive physical exam (IPPE).
- Patient consent: Patients must give written or verbal consent before billing. Consent is obtained once, unless the patient switches CCM providers. Consent should be documented.
- Comprehensive care plan: Maintain and update an electronic patient-centered care plan that includes the following:
- Physical, mental, and functional health assessments
- Caregiver and resource support inventory
- A copy provided to the patient and caregivers
- Electronic documentation for seamless provider access
- Clinical staff time: Each unit of 99439 requires documentation of at least 20 minutes of non-face-to-face clinical staff time per month under the direction of a physician or other qualified healthcare professional.
- Interactive communication: Services must include structured care coordination and ongoing patient communication, including phone calls or other (real-time) electronic interactions, like video calls, to support chronic care management.
- Access to care: Providers must ensure 24/7 patient access to clinical staff for urgent needs, continuity of care with a designated care team member, and secure communication via phone, messaging, or a patient portal.
Note: For a comprehensive guide on billing requirements for 99439 and the other CCM CPT codes, download this Chronic Care Management Coding and Billing Guide.
How Does 99439 Fit in With Other CCM CPT codes
CPT 99439 is an add-on code to CCM CPT code 99490, reimbursing additional clinical staff time for up to two additional units of 20 minutes beyond the initial 20-minute monthly threshold. Here is what that would look like for 60 minutes of time spent delivering CCM to a single patient in a month:

CPT codes 99439 and 99490 are part of the larger CCM billing structure. Below is a table identifying the set of CCM CPT codes with their descriptors, billing frequency, and time spent on care management.
|
CPT Code |
Descriptor |
Billing Frequency |
Time Spent |
|
99437 |
CCM services with the following required elements: multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient, chronic conditions that place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline, comprehensive care plan established, implemented, revised, or monitored. |
Monthly (add-on to 99491) |
Each additional 30 minutes by a physician or other qualified health care professional |
|
99439 |
CCM services with the following required elements: multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient, chronic conditions that place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline, comprehensive care plan established, implemented, revised, or monitored |
Monthly (add-on to 99490) |
Each additional 20 minutes of clinical staff time directed by a physician or other qualified health care professional |
|
99487* |
CCM services with the following required elements: multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient, chronic conditions that place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline, comprehensive care plan established, implemented, revised, or monitored, moderate or high complexity medical decision making. |
Monthly |
First 60 minutes of clinical staff time directed by a physician or other qualified health care professional |
|
99489* |
Complex chronic care management services with the following required elements: multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient, chronic conditions that place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline, comprehensive care plan established, implemented, revised, or monitored, moderate or high complexity medical decision making. |
Monthly (add-on to 99487) |
Each additional 30 minutes of clinical staff time directed by a physician or other qualified health care professional |
|
99490* |
CCM services with the following required elements: multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient, chronic conditions that place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline, comprehensive care plan established, implemented, revised, or monitored. |
Monthly |
First 20 minutes of clinical staff time directed by a physician or other qualified health care professional |
|
99491 |
CCM services with the following required elements: multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient, chronic conditions that place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline, comprehensive care plan established, implemented, revised, or monitored. |
Monthly |
First 30 minutes provided personally by a physician or other qualified health care professional |
*CPT codes 99487, 99489, and 99490 include time spent directly by the billing practitioners or clinical staff. Time spent by the billing practitioner may also count toward the time threshold if not used to report 99491.
**CPT code 99491 includes only time that’s spent personally by the billing practitioner. Clinical staff time does not count toward the required reporting time threshold code.
Pairing Other Care Management Programs With CPT 99439
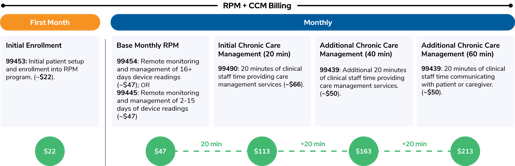
Providers frequently combine chronic care management with remote patient monitoring (RPM). The integration of RPM with CCM helps to ensure continuous monitoring fed by data from RPM devices, leading to improved health outcomes and increased revenue. From a coding perspective, RPM CPT code 99445 covers the device supply and 2-15 days of transmitted health data or CPT code 99454 covers the device supply and 16 days of transmitted health data, while CCM codes like CPT 99490 and 99439 reimburse for time spent reviewing data, adjusting treatment plans, and patient communication.
Here is what the described combination of RPM with 60 minutes of CCM looks like from a monthly coding and billing perspective:
Best Practices for CPT 99439
To best ensure chronic care management program efficiency, proper reimbursement, and ongoing compliance with CMS guidelines concerning the use of CPT 99439, practices with CCM programs should implement the following best practices:
- Proactively identify eligible patients early: Use EHR systems to flag CCM-qualified patients.
- Develop clear care plans: Tailor plans to individual patient needs and goals.
- Ensure proper documentation: Maintain current and accurate records to avoid audit and noncompliance risks.
- Utilize CCM software: Streamline workflows and track patient interactions efficiently.
- Patient engagement and education: Clearly communicate CCM benefits, encouraging patient participation.
Get More Out of Your CCM Program: Speak With a Prevounce Care Management Expert
Schedule a demo with Prevounce to see how our platform simplifies chronic care management coding and billing, improves CCM compliance, automates tracking, and helps providers achieve improved patient outcomes and financial performance. Book your demo today and take control of your care management program.
CPT Copyright 2025 American Medical Association. All rights reserved.
CPT® is a registered trademark of the American Medical Association.
Disclaimer
Health economic and reimbursement information provided by Prevounce is gathered from third-party sources and is subject to change without notice as a result of complex and frequently changing laws, regulations, rules, and policies. This information is presented for illustrative purposes only and does not constitute reimbursement or legal advice.
Prevounce encourages providers to submit accurate and appropriate claims for services. It is always the provider’s responsibility to determine medical necessity, the proper site for delivery of any services, and to submit appropriate codes, charges, and modifiers for services rendered. It is also always the provider’s responsibility to understand and comply with Medicare national coverage determinations (NCD), Medicare local coverage determinations (LCD), and any other coverage requirements established by relevant payers which can be updated frequently.
Prevounce recommends that you consult with your payers, reimbursement specialists, and/or legal counsel regarding coding, coverage, and reimbursement matters.
Payer policies will vary and should be verified prior to treatment for limitations on diagnosis, coding, or site of service requirements.