

Updated May 5, 2026
Update (Jan. 10, 2025): In the 2025 physician fee schedule final rule, CMS finalized the creation of Advanced Primary Care Management. Learn more about the new APCM program in our on demand webinar, "Crash Course on Advanced Primary Care Management."
* * *
One of the most noteworthy additions from CMS included in the 2025 physician fee schedule rule is the creation of an Advanced Primary Care Management (APCM) program. What makes this particular program so significant is that APCM is a complete reimagining of care management services in the primary care setting.
APCM demonstrates CMS's desire to further accelerate the movement away from fee-for-service and towards accountable and value-based care.
Let's dive into APCM further, including what it is, how it differs from other care management programs, its HCPCS codes, and how it concerns another new proposed concept called "Advanced Primary Care Hybrid Payments."
What is Advanced Primary Care Management (APCM)?
To further elaborate on what was shared above, an APCM program combines elements of existing care management programs, such as chronic care management (CCM) and principal care management (PCM). APCM incorporates select communications technology-based services (CTBS), such as virtual check-ins and remote evaluation of images, that have been introduced as separately billable services in recent years.
Unlike some existing care management programs, the APCM codes — which are provided below — are not time-based. Rather, they are broken out by patient risk and include 13 distinct "service elements," which are also discussed below.
CMS is hoping that APCM will expand the use of CCM services, which are presently underutilized through the fee-for-service model.
CMS's ultimate goal with APCM is to provide patients with a wider range of service options to meet individual needs while creating a unified code set for streamlined billing.
Advanced Primary Care Management HCPCS Codes
CMS has ruled APCM services can be furnished each calendar month by the practitioner assuming the care management role for a beneficiary. Here are the three APCM HCPCS codes, their descriptions, and their 2026 valuation.
HCPCS G0556 — APCM services for a patient provided by clinical staff and directed by a physician or other qualified healthcare professional who is responsible for all primary care and serves as the continuing focal point for all needed health care services, per calendar month. Valuation: $16 per patient per month
HCPCS G0557 — APCM services for a patient with multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient, which place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline, provided by clinical staff and directed by a physician or other qualified health care professional who is responsible for all primary care and serves as the continuing focal point for all needed health care services, per calendar month, with the elements included in G0556, as appropriate. Valuation: $54 per patient per month
HCPCS G0558 — APCM services for a patient that is a Qualified Medicare Beneficiary with multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient, which place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline, provided by clinical staff and directed by a physician or other qualified health care professional who is responsible for all primary care and serves as the continuing focal point for all needed health care services, per calendar month, with the elements included in G0556, as appropriate. Valuation: $117 per patient per month
Advanced Primary Care Management Service Elements
Now let's examine the 13 service elements that are required to bill each of the three HCPCS codes. These service elements, some of which overlap with chronic care management or principal care management services, must be "available" to patients, but not all service elements need to be provided each month.
1. Patient Consent
Inform the patient about the service, obtain consent, and document it in the medical record.
2. Initiating visit
For new patients or those not seen within three years.
3. Continuity of care
Ensure continuity with a designated team member for successive routine appointments.
4. Alternative care delivery
Care delivery options alternative to office visits, such as home visits and/or expanded hours.
5. Overall comprehensive care management
Conduct systematic needs assessments, ensure receipt of preventive services, manage medications and general clinical oversight.
6. Patient-centered care plan
Develop and maintain a comprehensive electronic care plan accessible to the care team and patient.
7. 24/7 access to care
Provide patients with 24/7 access to the care team/practitioner for urgent needs.
8. Coordination of care transitions
Coordinate transitions between healthcare settings and providers, ensuring timely exchange of health information and follow-up communication.
9. Ongoing communication
Coordinate with various service providers and document communications about the patient’s needs, goals, and preferences.
10. Enhanced communication opportunities
Enable communications through secure messaging, email, patient portals, and other digital means.
11. Population data analysis
Identify care gaps and offer additional interventions as appropriate.
12. Risk stratification
Use data to identify and target services to patients.
13. Performance measurement
Assess quality of care, total cost of care, and use of certified EHR technology.
Overlap With Existing Care Management Services
CMS acknowledges in the 2025 proposed rule that there are care management services/codes that are likely to be viewed as "substantially duplicative" of advanced primary care management service services and thus they would not be billable alongside APCM (i.e., must be one or the other).
These services, codes, and descriptions are as follows:
Chronic care management (CCM): CPT Codes 99487, 99489, 99490, 99491, 99439, 9943 — Management of all care for patients with two or more serious chronic conditions, timed, per month
Principal care management (PCM): CPT Codes 99424, 99425, 99426, 99427 — Management of all care for patients with one serious chronic condition, timed, per month
Transitional Care Management (TCM): CPT Codes 99495, 99496 — Management of transition from acute care or certain outpatient stays to a community setting, with face-to-face visit (bundled into payment for the code), once per patient within 30 days post-discharge
APCM and Remote Patient Monitoring
Medicare considered whether other care management services would be duplicative but decided that the likes of community health integration (CHI), SDOH, principal illness navigation (PIN) — all of which were new billable services for 2024 — and/or remote patient monitoring (RPM) or remote therapeutic monitoring (RTM) "may compliment" APCM services and thus could be billed on top of APCM.
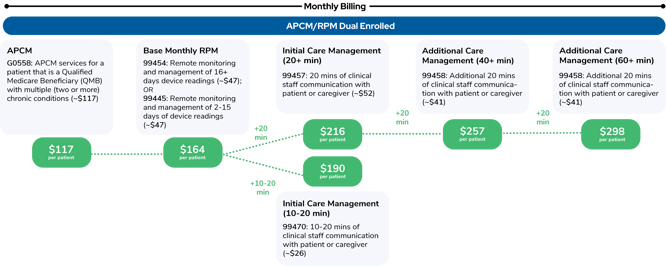
This provides an interesting incentive for currently dual-enrolled remote patient monitoring and chronic care management patients. Qualified care management time could conceivably be billed under RPM while the patient is enrolled in APCM since RPM time codes were not included in CMS’s list of duplicative services.
What might the coding and billing look like for a Qualified Medicare Beneficiary (QMB) dual-enrolled in an APCM and RPM program? Here's how it billing these two in 2026 looks:
Advanced Primary Care Hybrid Payment
Medicare believes that the new APCM code set "could serve as a chassis to incorporate primary care model learnings" into primary care services, according to the 2025 proposed rule. In the proposed rule, they requested comments on a new concept they call "Advanced Primary Care Hybrid Payments."
CMS states that APCM has five foundational components intended to "lay the path for a more transparent movement to value-based care." These elements are as follows:
- Streamlined value-based care opportunities
- Billing requirements
- Person-centered care
- Health equity, clinical, and social risk
- Quality improvement and accountability
CMS noted that it is "… seeking to create a stepping stone for primary care clinicians, including those new to value-based care, to move away from either encounters or other discrete components of overall care as the dominant method of primary care payment…"
To help make better decisions concerning this transition, CMS included a huge request for information (RFI) in the proposed rule. In total, CMS asked 47 questions intended to elicit feedback from stakeholders on the theme of moving the focus of primary care from evaluation and management (E/M) visits to value-based reimbursement.
Topics for feedback include:
- Streamlining value-based care opportunities and accountable care.
- How to bundle E/M services into APCM payments without disincentivizing visits
- How to structure payments to improve patient experience
- Aligning payment models with health equity and disadvantaged groups
- Balancing flexibility with accountability for patient outcomes
Note: 2025's proposed rule spent a significant amount of time contemplating and announcing a more concerted push towards accountable and value-based care. Releasing the APCM codes seems to be CMS putting the carrot first before tackling E/M bundling and other more disruptive moves CMS wants to make that would further move it away from the fee-for-service model.
Prevounce: A Leader in Remote Care Management
Looking for experts who can help you set up, operate, and manage a long-term successful remote care management program? Book a consultation with Prevounce today!
Want to Learn More? Download our Comprehensive Guide to APCM
To help you understand APCM, we published our "Comprehensive Guide to Advanced Primary Care Management." This expert resource builds the foundation of knowledge for starting an APCM program compliant with CMS guidelines, including: coding, billing, eligibility, compliance best practices, and complementary services. Download it here.